
 Download:
Download:




-
The onset of puberty is an important biological event in human growth and development. In recent years, a trend toward earlier pubertal onset has been observed among children and adolescents in China (1). Early pubertal timing increases the risk of cardiovascular diseases, such as obesity and hypertension in adulthood; however, research focusing on late adolescence is relatively limited (2). Meanwhile, the evaluation indicators for pubertal timing are mostly based on secondary sexual characteristics, with limited reports concerning age at take-off (ATO) and age at peak height velocity (APHV), which reflect characteristics of sudden increases in height (1). Therefore, using data from the Health Promotion Program for Children and Adolescents (HPPCA) in Suzhou, China (3), we conducted further analyses using ATO and APHV to evaluate the association between pubertal onset and adolescent obesity. Ultimately, 9,269 adolescents aged 15–17 years from 20 schools were enrolled, including 67,383 historical physical examination data from 2012 to 2020. In boys, early pubertal timing, as determined by ATO and APHV, was negatively associated with endpoint body mass index (BMI) and risk of obesity in late adolescence, independent of childhood BMI. APHV was inversely associated with endpoint BMI among girls. Our findings indicate that ATO and APHV can serve as early risk indicators of adiposity in adolescents. Thus, effective monitoring and management of pubertal development are essential, and preventive interventions should prioritize the reduction of childhood adiposity.
This study was a retrospective cohort analysis based on a large-scale, ongoing, school-based monitoring program from 2012 to 2020 in Suzhou City, Jiangsu Province, China. Detailed information about HPPCA has been previously published (3). In 2020, 19,824 students aged 15–17 years were selected from 20 schools. Height and weight were measured, and BMI was calculated by dividing weight (kg) by the square of height (m2). Additionally, 9,760 participants were excluded for the following reasons: fewer than four height measurements between 2012 and 2019; no height measurement at 6–8 years old; or fewer than three height measurements at 9–14 years old. Another 795 participants were excluded because of invalid values due to logical inconsistencies in fitting ATO and APHV. Ultimately, 9,269 adolescents, contributing 67,383 physical examination data points, were included in the study.
The Preece & Baines growth model, a set of nonlinear regression models proposed by Preece and Baines in 1978 to fit individual growth curves, was used to fit the ATO and APHV for each subject (4). By analyzing velocity (first derivative) and acceleration (second derivative), the model estimates the onset rate of sudden height increase, PHV, ATO, and APHV of individuals (4). Puberty timing onset was determined as early (
Categorical variables are presented as numbers and percentages, while continuous variables are reported as mean±standard deviation. In this study,t-tests and chi-square tests were used to compare differences between groups. We established initial participation in the HPPCA at 6–8 years of age as the baseline during 2012–2014 and designated the final measurement at 15–17 years of age (late adolescence) in 2020 as the endpoint. Linear and logistic regression models were used to analyze the associations of ATO and APHV with BMI levels and risks of obesity in late adolescence. We also analyzed the risks of elevated BMI levels and obesity in late adolescence for participants in the early group compared to the non-early group. Coefficients (β), odds ratios (ORs), and 95% confidence intervals (CIs) for the unadjusted model (Model 1) and the adjusted model (Model 2, adjusted for sex, area, age, and baseline BMI) were reported. The fitting of ATO and APHV was performed in Stata Statistical Software (version 16, Stata Corp., TX, USA) using the “pbreg” package. SPSS Statistics (version 22, IBM SPSS Inc., Chicago, IL, USA) was used for other analyses. AP-value of less than 0.05 was considered statistically significant.
The final analysis included 9,269 adolescents aged 15 to 17 years, comprising 4,857 boys (52.40%) and 4,412 girls (47.60%), with 5,212 urban (56.23%) and 4,057 rural (43.77%) participants. The ages at baseline and endpoint were 8.16±0.51 years and 15.96±0.50 years, respectively. The overall prevalence of obesity at baseline and endpoint was 14.79% and 10.18%, respectively, with a higher prevalence of obesity found in boys than in girls (P<0.05). The average number of follow-ups was 7.27±0.78. The ATO for girls was 7.93±2.19 years, occurring 1.24 years earlier than for boys (P<0.05). The APHV for girls was 10.75±1.22 years, which was 1.67 years earlier than for boys (P<0.05). Detailed general characteristics of the included children and adolescents are presented inTable 1. Additionally, the main characteristics of the included and excluded participants are outlined in
Supplementary Table S1 .Variable Total(n=9,269) Boys(n=4,857) Girls(n=4,412) t/χ2-value P Endpoint Age (years)* 15.96±0.50 15.95±0.50 15.96±0.50 −0.707 0.480 Height (cm)* 169.19±8.15 174.80±5.91 163.02±5.31 101.085 <0.001 Weight (kg)* 61.98±13.33 67.85±13.86 55.52±9.08 51.098 <0.001 BMI (kg/m2)* 21.56±3.79 22.17±4.18 20.88±3.19 16.773 <0.001 Area 0.292 0.589 Uran 5,212 (56.23) 2,744 (56.50) 2,468 (55.94) Rural 4,057 (43.77) 2,113 (43.50) 1,944 (44.06) BMI status 389.973 <0.001 Thinness 595 (6.42) 346 (7.12) 249 (5.65) Normal 6,182 (66.70) 2,816 (57.98) 3,366 (76.29) Overweight 1,548 (16.70) 996 (20.51) 552 (12.51) Obesity 944 (10.18) 699 (14.39) 245 (5.55) Numbers of follow−up* 7.27±0.78 7.27±0.79 7.26±0.78 0.559 0.576 ATO (years)* 8.58±2.24 9.17±2.13 7.93±2.19 27.582 <0.001 APHV (years)* 11.62±1.42 12.42±1.08 10.75±1.22 69.477 <0.001 Baseline Age (years)* 8.16±0.51 8.16±0.51 8.16±0.50 −0.137 0.891 Height (cm)* 130.32±5.98 130.98±5.95 129.59±5.94 11.261 <0.001 Weight (kg)* 28.84±5.96 29.99±6.33 27.58±5.24 20.019 <0.001 BMI (kg/m2)* 16.87±2.55 17.36±2.71 16.33±2.25 19.924 <0.001 Abbreviation: BMI=body mass index; ATO=age at take-off; APHV=age at peak height velocity.
* Continuous variables were presented as mean ± standard deviation.Table 1.General characteristics of enrolled children and adolescents [n(%)].
Table 2illustrates the associations between the onset of puberty timing and BMI and obesity in late adolescence. After adjusting for potential confounders, both ATO and APHV exhibited negative associations with endpoint BMI in late adolescence (β=−0.04, 95%CI: −0.07, −0.02;β=−0.17, 95%CI: −0.22, −0.12). ATO was negatively associated with obesity risk in late adolescence (OR=0.96, 95%CI: 0.93, 1.00). When stratified by gender, the association between ATO and endpoint BMI was only significant among boys. Similarly, ATO and APHV showed significant associations with obesity risks among boys but not girls.
Group BMI [β(95%CI)] Obesity [OR(95%CI)] Model 1 Model 2 Model 1 Model 2 ATO (age) Total 0.02 (−0.02, 0.05) −0.04 (−0.07, −0.02) 1.02 (0.99, 1.05) 0.96 (0.93, 1.00) Boys −0.17 (−0.23, −0.12) −0.08 (−0.12, −0.04) 0.93 (0.90, 0.96) 0.95 (0.90, 0.99) Girls 0.04 (0.00, 0.08) 0.00 (−0.03, 0.03) 1.03 (0.97, 1.10) 0.99 (0.92, 1.06) APHV (age) Total −0.15 (−0.20, −0.09) −0.17 (−0.22, −0.12) 1.00 (0.95, 1.05) 0.94 (0.87, 1.01) Boys −0.97 (−1.08, −0.87) −0.29 (−0.37, −0.21) 0.69 (0.64, 0.74) 0.90 (0.82, 0.99) Girls −0.33 (−0.41, −0.26) −0.07 (−0.12, −0.01) 0.83 (0.75, 0.92) 0.99 (0.88, 1.11) Note: Model 1: unadjusted, Model 2: adjusted for gender, area, age, and BMI at baseline.
Abbreviation: BMI=body mass index;β=coefficients;OR=odds ratio;CI=confidence interval; ATO=age at take-off; APHV=age at peak height velocity.Table 2.Associations of the onset of pubertal timing with BMI and obesity in late adolescence.
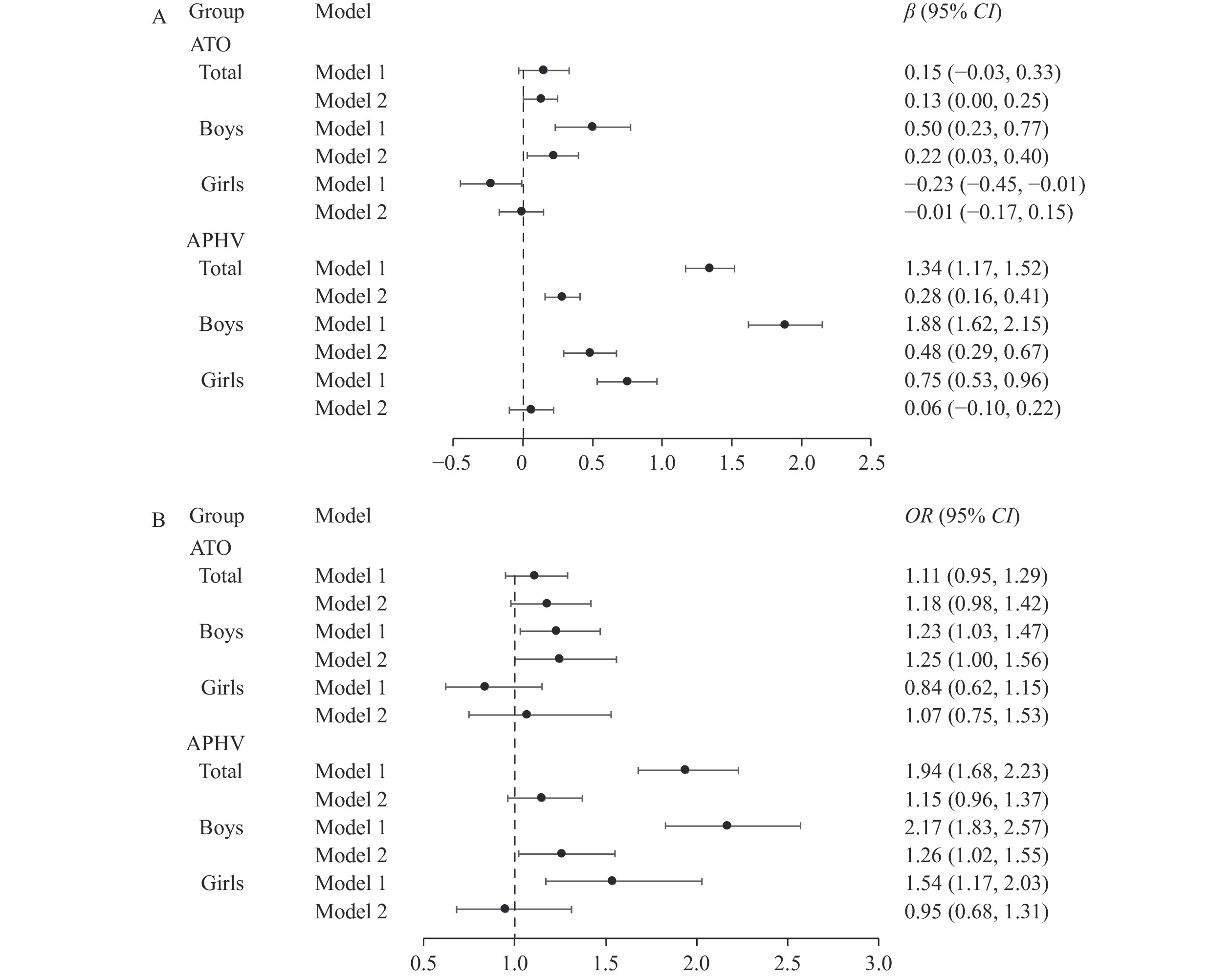
Compared with participants in the non-early group, those in the early group with earlier ATO and APHV exhibited higher BMI levels, with aβof 0.13 (95%CI: 0.00, 0.25) for ATO and 0.28 (95%CI: 0.16, 0.41) for APHV. For boys, these associations appeared stronger, with aβof 0.22 (95%CI: 0.03, 0.40) for ATO and 0.48 (95%CI: 0.29, 0.67) for APHV; however, no analogous patterns were observed among girls (P>0.05). Boys, but not girls, in the early-onset group identified by ATO and APHV had increased obesity risks than their counterparts in the non-early group, with anORof 1.25 (95%CI: 1.00, 1.56) for ATO and 1.26 (95%CI: 1.02, 1.55) for APHV.Figure 1includes more detailed information.
 Figure 1.
Figure 1.The risks of elevated BMI levels and obesity for participants in the early onset of pubertal timing group compared to those in the non-early group. (A) BMI levels. (B) Obesity.
Note: Model 1: unadjusted. Model 2: adjusted for gender, area, age, and BMI at baseline.
Abbreviation:β=coefficients;OR=odds ratio;CI=confidence interval; ATO=age at take-off; APHV=age at peak height velocity; BMI=body mass index.
-
This study used the Preece & Baines growth model to fit height data from 9,269 children and adolescents collected from 2012 to 2020. This model facilitated the construction of a height development curve and calculation of ATO and APHV. The results showed that the average ATO for boys and girls in Suzhou was 9.17 years and 7.93 years, respectively, while the average APHV was 12.42 years and 10.75 years, respectively. Notably, sex differences were observed in the associations between early pubertal timing and late adolescence obesity. In boys, both ATO and APHV were negatively correlated with the risk of obesity in late adolescence, independent of childhood BMI. Conversely, no similar associations were found in girls.
A study including 28,251 adolescents in Changzhou City, Jiangsu Province, China, reported that ATO was 9.3 years for boys and 8.0 years for girls, while APHV was 12.6 years for boys and 10.6 years for girls (5). Chen et al. analyzed 13,143 children in a longitudinal cohort from 2006 to 2016 in Zhongshan City, Guangdong Province, and found that ATO was 7.9 and 9.1 years in girls and boys, respectively, and APHV was 10.8 years in girls, 1.9 years earlier than in boys (6). The findings of this study align with other regional data within China. Nevertheless, they show some discrepancies compared with data from other countries. A cohort study of 7,495 US children investigated early-life growth patterns and the age at pubertal onset, revealing APHV values of 12.9 years for boys and 10.8 years for girls (7). Additionally, a study aimed at estimating the height growth curve for Mexican children, involving 7,097 boys and 6,167 girls, found that ATO and APHV were 8.6 and 12.4 years for boys, respectively, and 7.0 and 9.9 years for girls, respectively (8). The observed variations are potentially due to differences in the timing of selection, ethnicity, environmental factors, and socioeconomic status of the participants.
Research on the associations of pubertal timing with obesity, based on ATO and APHV, is limited, especially in late adolescence. Limited research indicates that advanced APHV is associated with increased BMI levels in late puberty and adulthood. A cohort study by Chen et al. (6) showed that early APHV (RR=1.16, 95%CI: 1.03, 1.30) was associated with an increased risk of overweight and obesity in late adolescence. While this study found a negative correlation between girls’ APHV and BMI in late adolescence, there was no statistically significant correlation of ATO and APHV with the risk of obesity. This finding aligns with the results of O'Keeffe et al. (9); however, Chen et al. (6) reported an increased risk of obesity associated with APHV in girls, indicating inconsistencies across studies. These discrepancies may stem from various factors, including different growth modeling methods, such as the SITAR model, Preece-Baines growth model, and growth curves. Even when employing the same model, variations in sample size, number of measurements, data balance, and measurement errors can lead to fitting deviations. Furthermore, the continuous nature of nutritional status throughout different life stages and the link between childhood obesity and the premature onset of puberty must be considered. Failing to account for pre-pubertal nutritional status could lead to misinterpretations of the associations between ATO, APHV, and obesity during late puberty. Thus, further research is necessary to elucidate the links between ATO, APHV, and obesity in late adolescence and adulthood. Additionally, this study found gender-specific associations between pubertal onset and adolescent obesity. Gender differences in this association may be attributed to sexual dimorphism in fat distribution and metabolism, coupled with a robust synergistic relationship between estrogen and leptin in the regulation of reproductive and energy homeostasis (6).
Based on the Chinese National Survey on Students Constitution and Health, the prevalence of obesity in 2019 was 9.6% among children and adolescents aged 7~18 years, with 11.9% in children aged 7~8 years and 6.7% in adolescents aged 15~17 years in China. The prevalence of obesity among participants in this study was higher than the national average, consistent with trends in eastern China (10). This emphasizes that obesity is a major public health concern, particularly in coastal and economically developed areas. Given these findings, when boys present with early rapid height growth, healthcare providers should prioritize their nutritional status and implement health education and lifestyle interventions, including dietary modifications, exercise, and behavioral changes.
This study has several limitations. First, because participants were exclusively from Suzhou, China, caution is warranted when extrapolating these findings to other populations. Differences in ethnicity, living environments, and socioeconomic levels may influence the results. Second, the research design did not account for potentially significant confounding factors, including genetic influences; pregnancy and childbirth information; early-life exposures; and lifestyle factors such as diet, exercise behaviors, and sleep patterns. These omissions could affect the study's conclusions regarding the associations between the timing of puberty onset and obesity.
-
All the children, parents, and workers who were involved in this study.
HTML
| Citation: |

|