
 Download:
Download:




-
Hainan Island, a tropical province in China, is situated in the “Tsutsugamushi Triangle Area” and is known for being an endemic region for ST, rickettsioses, and related diseases. From 2009 to 2011, the prevalence rates of ST and rickettsioses [spotted fever group (SFG) and typhus group (TG)] among undifferentiated febrile illness (UFI) patients in Hainan were reported as 5.5% and 5.9%, respectively (1). Initially considered endemic mainly to southern China, ST has increasingly spread northward, with a notable rise in national case numbers from 1,375 in 2006 to 23,474 in 2017 (2). Clinical features of ST and rickettsioses show similarities to other rickettsia-like diseases, including anaplasmosis, ehrlichiosis, Q fever, and chlamydiosis, as well as various bacterial, viral, and parasitic infections like influenza, malaria, and Lyme disease (3). Despite this, the involvement of these rickettsia-like pathogens in UFI remains to be thoroughly investigated.
We previously developed a TaqMan PCR array to identify bacterial pathogens in patients with UFI from Inner Mongolia Autonomous Region, China (4). In this study, we expanded our investigation to include the detection of 9 significant bacterial pathogens —Orientia tsutsugamushi,Rickettsiaspp.,Anaplasma phagocytophilum,Ehrlichia chaffeensis,Coxiella burnetii,Chlamydia psittaci,Brucellaspp.,Burkholderia pseudomallei, andBorrelia burgdorferi— in UFI patients treated in Haikou City, Hainan Province between 2018 and 2021. Our findings highlight the current patterns of ST and rickettsioses in Hainan, as well as the prevalence of co-infections involvingO. tsutsugamushiandA. phagocytophilumin China.
-
Blood samples and demographic data were obtained from 503 UFI outpatients at the Affiliated Hospital of Hainan Medical School between June 2018 and August 2021. Blood from putative ST patients (n=13), along with their eschar swabs (n=6) samples were provided by the Center for Disease Control and Prevention of Guangxi in September 2020. In June 2021, 624 blood samples from healthy volunteers in Yunnan Province were collected by the Institute of Endemic Diseases Control and Prevention of Yunnan. DNA extraction was performed according to standard protocols (4).
The primer and probe sequences were detailed in
Supplementary Table S1 . TaqMan PCR arrays were carried out as previously described (4). Primary screening utilized pooled samples (n=5) based on experimental validation. Pools with Ct values <40 in the initial screening underwent individual testing to identify positive cases. A Ct value of ≤35 was considered positive, Ct values between 35 and 40 were considered putative positive, and Ct values ≥40 were considered negative (4). -
TaqMan PCR positive samples (Ct≤35) were confirmed through verification using nested PCR and subsequent amplicon sequencing. The nested PCR reaction included 10 µL of 2× TSINGKE Master Mix, 2.5 µL of each forward and reverse primer (10 µmol/L), 2 µL of the template, made up to 25 µL with water. PCR cycling was carried out on a Thermo-Cycler from SensoQuest GmbH., Germany, involving an initial denaturation step at 98 ℃ for 5 min, 30 cycles of 94 ℃ for 20 s, 50 ℃ for 20 s, and 72 ℃ for 20 s, and a final extension at 72℃ for 10 min. The products from the first PCR round (2 µL) were utilized as templates for the subsequent PCR round. Amplicons from the nested PCR were assessed on a 1% agarose gel before sequencing (Tsingke Biotechnology Co. Ltd.). Phylogenetic trees were generated using MEGA 10.1.8.
-
We utilized SPSS software (version 25.0, IBM, NewYork, USA) to conduct statistical analysis (4). The Pearson’s chi-squared test was employed to assess the differences in incidences based on age, gender, and occupation. Statistical significance was determined atP<0.05.
-
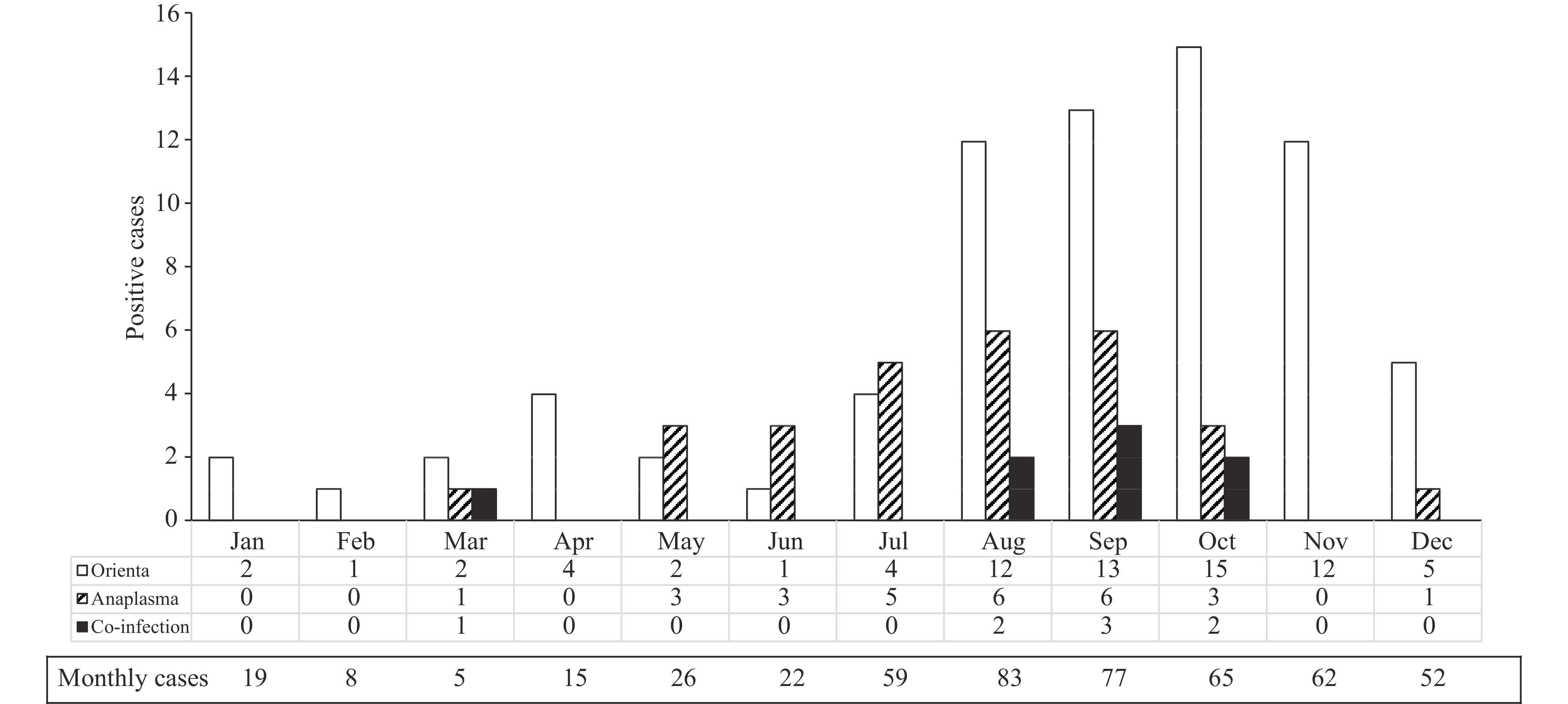
Among 503 patients with UFI, they were from 17 out of 18 counties in Hainan Island. A total of 73 (14.51%) and 28 (5.57%) were positive forO. tsutsugamushiandA. phagocytophilum, respectively (Table 1).O. tsutsugamushiinfections were detected year-round, peaking from September to October (Figure 1). Farmers had the highestO. tsutsugamushiinfection rate, while adolescents showed a higherA. phagocytophiluminfection rate. Co-infection withO. tsutsugamushiandA. phagocytophilumwas observed in 1.59% (8/503) of the UFI patients, mainly from August to October (Figure 1). Notably, other pathogens includingRickettsiaspp.,E. chaffeensis,C. burnetii,C. psittaci,Brucellaspp.,B. pseudomallei, andB. burgdorferiwere not detected in these UFI patients.
Variables Patient No. Anaplasma phagocytophilum Orientia tsutsugamushi Co-infection* Positive† Positive rate (%) Positive Positive rate (%) Positive Positive rate (%) No. No. No. Gender§ Male 320 20 6.25 48 15 1 0.31 Female 183 8 4.37 25 13.67 7 3.83 Age, years <20 25 4 16 3 12 0 — 20–29 44 0 — 2 4.54 0 — 30–39 78 4 5.13 10 12.82 0 — 40–49 86 8 9.3 14 16.28 4 4.65 50–59 86 4 4.65 15 17.44 1 1.17 60–69 98 5 5.1 15 15.3 2 2.04 70–79 61 1 1.64 11 18.03 1 1.64 Unknown 25 2 8 3 12 0 — Occupation§ Student 21 3 14.29 3 14.29 0 — Farmer 185 13 7.03 36 19.46 6 3.24 Retirement 35 1 2.86 6 17.14 1 2.85 Worker 53 2 3.77 7 3.21 0 — Self-employed 9 0 — 0 — 0 — Unknown 200 9 4.5 21 10.5 1 0.05 Note: “−” means positive rate cannot be calculated.
Abbreviation: UFI=Undifferentiated Febrile Illness.
* Co-infection withOrientia tsutsugamushiandAnaplasma phagocytophilum.
†TaqMan PCR Ct<40.
§Gender and occupational distribution of co-infection were statistically significant (P<0.05).Table 1.Prevalence ofAnaplasma phagocytophilumandOrientia tsutsugamushiin patients with UFI from Hainan Province, China, between 2018 and 2021.
 Figure 1.
Figure 1.Month-wise distribution of positive cases ofOrientia tsutsugamushi,Anaplasma phagocytophilum, and co-infection in Hainan, 2018–2021.
To further investigate co-infection, we collected blood samples from 13 clinically suspected ST patients and 6 eschar samples in the Guangxi Zhuang Autonomous Region. All 13 blood samples tested positive forO. tsutsugamushi(
Supplementary Table S2 ). Surprisingly, 61.5% of these ST patients also tested positive forA. phagocytophilum, indicating a high co-infection rate. While eschars are typically associated withO. tsutsugamushiinfection in ST-endemic regions, 3 out of the 6 eschar samples tested positive forA. phagocytophilum, suggesting a potential shared vector. Additionally, we found a co-infection rate of 0.48% (3/624) in blood samples from apparently healthy volunteers in Yunnan. The positivity rates forO. tsutsugamushi,A. phagocytophilum, andRickettsiaspp. were 8.97% (56/624), 3.69% (23/624), and 2.88% (18/624), respectively. -
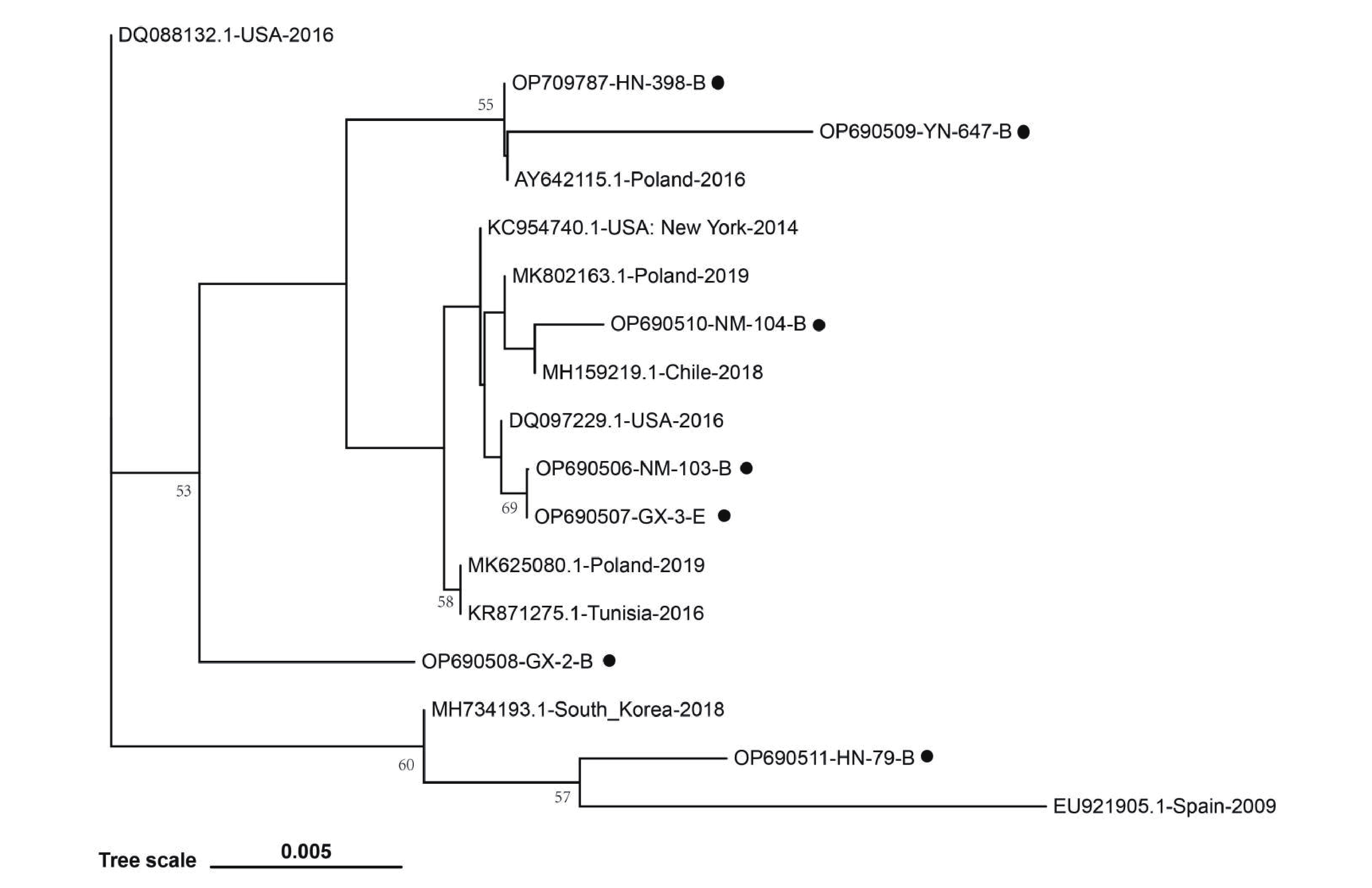
TaqMan PCR positive samples (Ct≤35) forO. tsutsugamushiorA. phagocytophilumunderwent further validation using nested PCR and sequencing. The sequences obtained were assigned GenBank accession numbers: OP698261–OP698267 for the partial 56-kDa gene ofO. tsutsugamushiand OP690506–OP690511 along with OP709787 for the partialmsp2 gene ofA. phagocytophilum. These sequences were aligned via the Basic Local Alignment Search Tool (BLAST) and subjected to analysis using MEGA 10.1.8 software. A phylogenetic tree constructed based on the partialmsp2sequences demonstrated genetic diversity amongA. phagocytophilumstrains in Hainan, Yunnan, Guangxi, and Inner Mongolia provincial-level administrative divisions (PLADs) (Figure 2). Notably, a distinct genetic branch comprising isolates OP690506 and OP690510 from Inner Mongolia, OP690507 and OP690508 from Guangxi, OP690509 from Yunnan, and OP709787 from Hainan appears to be predominant inA. phagocytophiluminfections in China. Furthermore, isolate OP690511 from Hainan clustered separately, suggesting the co-circulation of differentA. phagocytophilumstrains on Hainan Island.
 Figure 2.
Figure 2.Phylogenetic analysis of the partial msp 2 sequences of Anaplasma phagocytophilum amplified from patients with undifferentiated febrile illness in Hainan (HN), Inner Mongolia (NM), Guangxi (GX), and apparent healthy population in Yunnan (YN).
-
In this study, nine bacterial pathogens were investigated using a previously established TaqMan PCR array in patients with UFI in Hainan Province, where ST and rickettsioses have historically been prevalent. Among the tested samples,Orientia tsutsugamushiwas detected in 14.51% (73/503), representing a more than 2-fold increase compared to the prevalence in 2009–2011 (5.5%, 13/236) (1). ST remains the top and ever-increasing threat to the population of Hainan. The increased incidence of ST could be due to the different sensitivities of the TaqMan PCR used in this study and the nested PCR used in the previous study (1), but is more likely attributable to changes in environmental factors such as temperature and rainfall (5). Previous studies have reported seroprevalences of TGRickettsia(11.4%, 27/236) in Hainan (6). Surprisingly,Rickettsiaspp. were not detected in the present study, although the conserved 17-kDa protein gene ofRickettsiasibiricawas successfully used as a target for the detection ofRickettsiaspp. (SFG/TG) in clinical samples from Yunnan (in this study) and Inner Mongolia PLADs (4). In contrast, the incidence of TG infection in UFI in 2009–2011 was 5.9% (14/236) (1). This decline in rickettsioses could be attributable to rapid urbanization in Hainan over the last decade and the associated reduction in exposure to fleas and rats, which are the vectors and hosts of TG, respectively. Although further investigation and continuous monitoring are needed, the current results illustrate a shift in the epidemic trends of ST and rickettsioses in Hainan. It is worth noting that only 2 out of the 9 tested pathogens were detected in the UFI patients from Hainan. However, positive infections ofEhrlichia chaffeensis,Borrelia burgdorferi,Coxiella burnetii,Chlamydia psittaci,Brucellaspp., andBurkholderia pseudomalleihave previously been documented in the Hainan region (6–10). Therefore, caution should be exercised when interpreting the current results. Although our data imply that the undetected pathogens may play minor roles in UFI patients, the potential risk of these pathogens cannot be ruled out due to the biased sample size collected each year and the limitations of the TaqMan PCR array employed in this investigation. It is recommended that alternative primer-probe sets of targeting genes for the TaqMan array be tested to validate the results. In addition, cutting-edge technologies such as next-generation sequencing-seminested recombinase polymerase amplification assay (snRPA-nfo) will be of great help in identifying pathogens from clinical samples (11).
Anaplasmosis is a tick-borne disease present throughout China. A study in Hainan reported a highA. phagocytophilumseropositivity rate of 39.2% (337/852) among individuals tested (6). This could be attributed to the prolonged presence of IgG antibodies againstOrientia,Rickettsia, orAnaplasma, commonly found in both recovering patients and asymptomatic carriers (12). In the current investigation, 5.57% (28/503) of UFI patients tested positive forA. phagocytophilum. Hence, local health authorities should considerA. phagocytophiluminfection in UFI cases.
Simultaneous infections withA. phagocytophilumandB. burgdorferi,O. tsutsugamushi, and Thrombocytopenia Syndrome virus have been documented (13–15). Co-infections pose a new public health challenge that often goes overlooked. Apart from cases identified in Taiwan, China (14), instances of co-infection withO. tsutsugamushiandA. phagocytophilumhave been confirmed in Hainan (10.96%, 8/73 patients), Guangxi (61.5%, 8/13 patients), and Yunnan (5.36%, 3/56 positive population) PLADs of China. Notably, serological evidence of co-infection was found in suspected individuals from The Republic of Korea (2.9%, 8/274) (15). While current and past research highlights the prevalence of co-infection in South Asia, larger studies are needed to verify its extent across the Tsutsugamushi Triangle Area.
In conclusion, our findings provide insight into the ongoing epidemic patterns ofrickettsialandrickettsia-like diseases in Hainan. Moreover, they underscore the significant public health risk posed by co-infections involvingO. tsutsugamushiandA. phagocytophilumin China.
-
No conflicts of interest.
-
The authors wish to acknowledge all the donors, medical lab and administrative personnel of the Affiliated Hospital of Hainan Medical School for their help in sample collection. We would like to thank the colleagues in the departments or groups of ICDC for kindly providing reference DNA for this study.
HTML
Sample Collection, DNA Extraction, and TaqMan PCR Screening
Nested PCR and Amplicon Sequencing
Statistical Analysis
Detection of Pathogens in Clinical Samples
Sequence Comparison and Phylogenetic Analysis
CONCLUSIONS
| Citation: |

|