
 Download:
Download:




-
On June 4, 2023, a child presenting with severe melioidosis was admitted to Beijing Children’s Hospital, a tertiary teaching hospital. The child developed a fever after contact with contaminated water while traveling in Thailand, and later returned to China seeking treatment. Over the course of a three-month treatment period, the patient tragically Suffered from fatal septic shock, acute respiratory distress syndrome (ARDS), and acute kidney injury (AKI). This case underscores the need for vigilance regarding melioidosis in non-endemic regions, particularly with the increase in tourism.
-
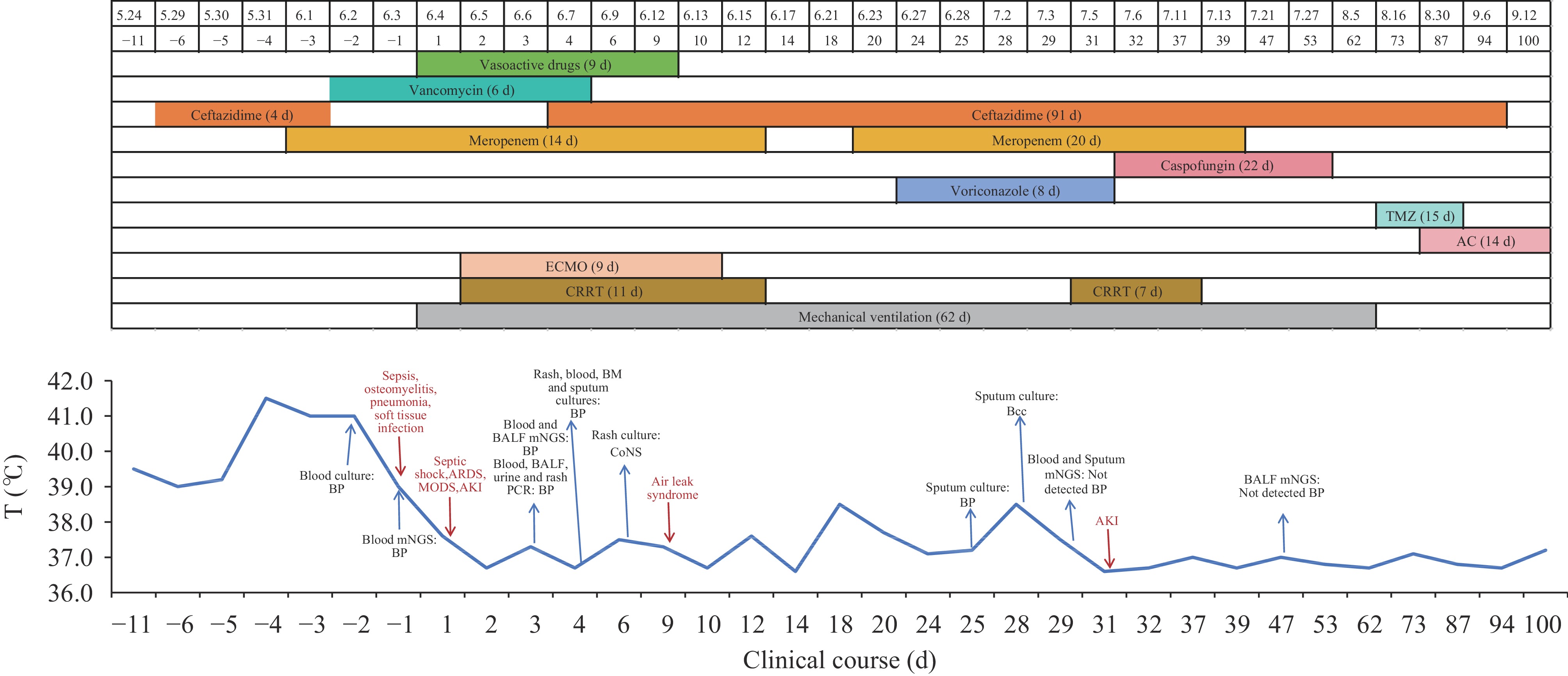
A six-year-old previously healthy boy was stung by a jellyfish on May 24, 2023, while vacationing in Thailand. The following day, his wounded foot was exposed to contaminated water in a jungle, after which he developed a fever. That evening, he returned to Liaoning Province. On May 29, he exhibited high fever and was treated with intravenous ceftazidime at a tertiary hospital in Dalian without a definitive diagnosis. Still febrile on May 30, he was transferred to a second tertiary hospital in Dalian, where he was diagnosed with pneumonia and continued on ceftazidime. By June 1, his condition deteriorated, marked by paroxysmal dry cough and red papules with central pus points. Imaging revealed multiple inflammatory nodules in both lungs and abscesses in both lower limbs. Following a sepsis diagnosis, his treatment was escalated to meropenem. Blood cultures taken on May 30 and processed at the second hospital identifiedBurkholderia pseudomallei(BP), sensitive to cefotaxime and meropenem, prompting continued meropenem therapy. On June 3, BP was confirmed via metagenomics next-generation sequencing (mNGS) of peripheral blood, with no other pathogens detected. The situation worsened, and on June 4, he was treated in the emergency department of Beijng Children’s Hospital, where he developed circulatory collapse and was admitted to the pediatric intensive care unit (PICU). Beijing CDC was notified of the case the same day. Subsequent polymerase chain reaction (PCR) testing of the patient’s blood, bronchoalveolar lavage fluid (BALF), urine, and pus confirmed sustained BP infection, with cultures from BALF and pus supporting these findings. The patient required mechanical ventilation, extracorporeal membrane oxygenation (ECMO), and continuous renal replacement therapy (CRRT) for ARDS, refractory septic shock, and AKI. During his stay, he received a prolonged course of meropenem (31 days) and ceftazidime (91 days), which effectively controlled the BP infection. Maintenance therapy with Trimethoprim-sulfamethoxazole (TMZ) began on August 16, but was switched to Amoxicillin-clavulanate (AC) on August 30 due to renal dysfunction. The patient was discharged on September 12, and fully recovered (Figure 1).
 Figure 1.
Figure 1.Timeline of the patient’s clinical course and detection results.
Note: The negative sign on the abscissa means “the day before admission”.
Abbreviation: BALF=bronchoalveolar lavage fluid; BM=bone marrow; CoNS=coagulase-negative staphylococci; Bcc=Burkholderia cepacia complex.
-
Melioidosis is a lethal infectious disease resulting from infection by BP. The risk of contracting this disease increases significantly with exposure to soil and water contaminated by BP. Predominantly, this disease occurs within the 20° north and south latitudes, exhibiting the highest incidence rates in Thailand and Australia. In China, the southern provincial-level administrative divisions (PLADs) such as Hainan, Guangdong, and Guangxi are identified as high-risk areas for melioidosis (1).
Although relatively rare, BP remains a significant travel-related disease. Approximately 40.8% of international travelers diagnosed with melioidosis have traveled to Thailand (2). Between 2016 and 2022, China reported 4 cases of melioidosis linked to international travel (2), along with several instances of BP associated with domestic travel within the country (3). In our increasingly globalized world, the movement of people and goods has facilitated the dissemination of BP (4).
In regions not commonly affected by epidemics, diagnosing melioidosis presents significant challenges: 1) Clinical laboratory tests: While the culture of specimens is considered the definitive diagnostic criterion for BP infection, its sensitivity is only about 60.2% (5). The early detection of BP via antigen and antibody testing is also problematic in non-epidemic areas. 2) Clinical manifestations: The symptoms of melioidosis are non-specific and can lead to misdiagnoses such as pneumonia, sepsis, or tuberculosis (6). Consequently, a complete recording of characteristic symptoms may not occur (7). Furthermore, there is considerable variation in the onset of symptoms among patients. Reports indicate that 55.4% of patients show symptoms within one week, while 28.6% may not exhibit any symptoms until 12 weeks post-exposure. Hence, diagnosis of melioidosis in travelers could be delayed by up to 18 months from the initial onset of symptoms (2). These factors collectively hinder the timely and effective diagnosis and treatment of melioidosis in non-endemic regions.
Given that the mortality rate of melioidosis can reach 73.7% among blood culture-positive patients during hospitalization (2), early identification of pathogens and provision of targeted treatment are crucial. mNGS, known for its time efficiency and high sensitivity, may be utilized for the early detection of such pathogens, potentially enhancing the identification and management of rare pathogens and infectious diseases.
Severe melioidosis progresses rapidly and requires multifaceted treatment approaches. In this case, the patient’s condition worsened swiftly during the initial phase of the illness, necessitating a transition to meropenem as the preferred antibiotic. Unfortunately, the sole use of antibiotic therapy proved inadequate at this critical stage, underscoring the necessity for simultaneous life-supportive therapies. Consequently, health departments and healthcare professionals must prioritize early detection and intervention in melioidosis to avert its progression to a severe form.
This case of imported melioidosis in a non-epidemic region underscores the need to improve risk assessments for travel-related infectious diseases. As the coronavirus disease 2019 (COVID-19) epidemic subsides, tourist numbers are likely to surge. Consequently, it is crucial to offer health education to individuals traveling to regions with a high prevalence of infectious diseases. Additionally, healthcare providers must be vigilant about patients’ travel histories and improve their capacity to identify and diagnose potential travel-related cases.
-
No conflicts of interest.
HTML
| Citation: |

|