
 Download:
Download:




-
Persistent infection with high-risk human papillomavirus (HPV) leads to invasive cervical cancer (1-2). The World Health Organization calls for the elimination of cervical cancer through HPV vaccination, screening for progressive cervical intraepithelial neoplasia (CIN), and early treatment (3). Understanding the prevalence of high-risk HPV types in CIN cases can inform prevention strategies. Prevalence data, however, has not been updated in China since 2009 (4). This clinically multicentric study investigated the HPV prevalence in CIN cases in 2017–2018, which was prior to the introduction of HPV vaccines in the mainland of China. The results showed that more than 90% of CIN2/3 cases were in individuals positive for high-risk HPV. In particular, HPV-16/18 were significantly associated with an increased risk of high-grade lesions. This study provides evidence to inform HPV-based screening and vaccination strategies and suggests that HPV-16/18 prevention should be prioritized.
From March 2017 to October 2018, the study recruited women aged 20–64 years old who exhibited abnormalities during screenings or had genital tract symptoms. We selected eight tertiary hospitals or maternal and child healthcare hospitals from 7 provincial-level administrative divisions (PLADs) including Beijing, Shanxi, Shannxi, Jiangsu, Hunan, Guangdong, and Chongqing according to the geographic distribution and burden of cervical cancer in China. These hospitals were local centers for cervical prevention and treatment and were the designated hospitals for referred patients in a prior population-based screening (5). A clinician interviewed patients with a structured questionnaire and collected information on demographic characteristics, the history of screening and diseases, and genital symptoms. Then a cervical specimen was obtained by the clinician with a brush and stored in a reserve (Hologic, Bedford, MA, USA) for HPV testing and cytology examination. Cobas HPV assay (Cobas 4800, Roche Molecular Systems, Pleasanton, CA, USA) was used and reported for HPV-16, -18, and 12 other non-16/18 high-risk types (including HPV-31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68). Liquid-based technology (ThinPrep, Hologic, MA, USA) was used to generate slides for cytology examination. A panel of cytotechnicians examined these slides under the microscope and reported the results according to the Bethesda terminology. A skilled cytologist selected all the positive slides and randomly selected 20% of negative slides to review the results.
Each patient underwent a colposcopy examination, colposcopy-directed four-quadrant biopsy, histological confirmation, and endocervical curettage. Two pathologists from local hospitals reviewed the pathological sections and reported the results according to the CIN terminology. Two skilled pathologists independently reviewed the results to avoid false-negative or false-positive results. This study included cases with CIN grades 1, 2, and 3, and adenocarcinoma in situ (AIS). We classified AIS as CIN3 and defined CIN2/3 as high-grade lesions.
We estimated the overall and age-specific prevalence of high-risk HPV in all CIN cases and CIN2/3 cases, respectively. Fisher’s exact method was used to estimate 95% confidence intervals (CI). To show the age-specific trends of HPV prevalence in CIN2/3, we used generalized additive models with quasibinomial distribution, adjusting for region and smoking status. Furthermore, we evaluated the association of different HPV infection patterns with high-grade CIN by multivariate ordinal or binomial logistic regression, adjusting for age, region, and smoking status. The former regarded the outcome as an ordinal variable, whereas the latter regarded CIN1 and CIN1/2 as reference groups, respectively. All analyses were done with SAS (version 9.4; SAS Institute, Cary, USA) and R software (version 3.5.3; R Foundation for Statistical Computing, Vienna, Austria).
There were 1,480 histologically confirmed CIN cases tested with HPV infection status, including 740 CIN1, 396 CIN2, and 344 CIN3 (Table 1). The median age was 37.6 years old for all CIN cases. The prevalence of 14 high-risk HPV types in all CIN cases was 85.1% (95%CI: 83.2%–86.9%). The prevalence of all HPV types and HPV-16/18 prevalence in CIN2/3 cases were 92.2% (95%CI: 90.0%–94.0%) and 52.0% (95%CI: 48.4%–55.7%), respectively, which is higher than in CIN1 cases (78.0%, 95%CI: 74.8%–80.9% and 25.4%, 95%CI: 22.3%–28.7%). In contrast, the prevalence of non-16/18 high-risk HPV types in CIN1 was 64.3%, 95%CI: 60.8%–67.8%), which was higher than in CIN2/3 (56.6%, 95%CI: 53.0%–60.2%). There were 50 cases with invalid cytology results. Among CIN2/3 cases with HPV positive results, 4.9% were classified as normal cytology, and these cases mostly occurred in those who were positive for non-16/18 HPV types.
HPV types All CIN (n=1,480) CIN 1 (n=740) CIN 2 (n=396) CIN 3 (n=344) CIN2/3 (n=740) Pfor CIN2/3
vs. CIN1n Prevalence
(95%CI)n Prevalence
(95%CI)n Prevalence
(95%CI)n Prevalence
(95%CI)n Prevalence
(95%CI)All HPV+ 1,259 85.1 (83.2–86.9) 577 78.0 (74.8–80.9) 358 90.4 (87.1–93.1) 324 94.2 (91.2–96.4) 682 92.2 (90.0–94.0) <0.001 Normal 106 7.2 (5.9–8.6) 70 9.5 (7.5–11.6) 24 6.1 (3.9–8.9) 12 3.5 (1.6–5.4) 36 4.9 (3.4–6.7) <0.001 ASC–US or worse 1,120 75.7 (73.5–77.9) 489 66.1 (62.5–69.5) 328 82.8 (78.8–86.4) 303 88.1 (84.2–91.3) 631 85.3 (82.5–87.8) <0.001 HPV-16 496 33.5 (31.1–36.0) 137 18.5 (15.8–21.5) 165 41.7 (36.8–46.7) 194 56.4 (51.0–61.7) 359 48.5 (44.9–52.2) <0.001 Normal 36 2.4 (1.7–3.4) 17 2.3 (1.3–3.7) 11 2.8 (1.4–4.9) 8 2.3 (1.0–4.5) 19 2.6 (1.6–4.0) 0.745 ASC–US or worse 452 30.5 (28.2–33.0) 119 16.1 (13.5–18.9) 152 38.4 (33.6–43.4) 181 52.6 (47.2–58.0) 333 45.0 (41.4–48.7) <0.001 HPV-18 92 6.2 (5.0–7.6) 57 7.7 (5.9–9.9) 22 5.7 (3.5–8.3) 13 3.8 (2.0–6.4) 35 4.7 (3.3–6.5) 0.018 Normal 15 1.0 (0.5–1.5) 11 1.5 (0.7–2.6) 4 1.0 (0.3–2.6) NA NA 4 0.5 (0.2–1.4) 0.069 ASC–US or worse 71 4.8 (3.8–6.0) 42 5.7 (4.1–7.6) 17 4.3 (2.5–6.8) 12 3.5 (1.8–6.0) 29 3.9 (2.6–5.6) 0.114 Other HPV types 895 60.5 (57.9–63.0) 476 64.3 (60.8–67.8) 237 59.9 (54.8–64.7) 182 52.9 (47.5–58.3) 419 56.6 (53.0–60.2) 0.002 Normal 69 4.7 (3.7–5.9) 50 6.8 (5.1–8.8) 13 3.3 (1.8–5.6) 6 1.7 (0.6–3.8) 394 2.6 (1.6–4.0) <0.001 ASC–US or worse 804 54.3 (51.8–56.9) 410 55.4 (51.7–59.0) 221 55.8 (50.8–60.8) 173 50.3 (44.9–55.7) 19 53.2 (49.7–56.8) 0.404 HPV-16/18 573 38.7 (36.2–41.3) 188 25.4 (22.3–28.7) 184 46.5 (41.5–51.5) 201 58.4 (53.0–63.7) 385 52.0 (48.4–55.7) <0.001 Normal 49 3.3 (2.5–4.4) 26 3.5 (2.3–5.1) 15 3.8 (2.1–6.2) 8 2.3 (1.0–4.5) 23 3.1 (2.0–4.6) 0.663 ASC–US or worse 510 34.5 (32.0–36.9) 157 21.2 (18.3–24.3) 166 41.9 (37.0–47.0) 187 54.4 (48.9–59.7) 353 47.7 (44.1–51.3) <0.001 Other HPV types (no 16/18) 686 46.4 (43.8–49.0) 389 52.6 (48.9–56.2) 174 43.9 (39.0–49.0) 123 35.8 (30.7–41.1) 297 40.1 (36.6–43.7) <0.001 Normal 57 3.9 (2.9–5.0) 44 6.0 (4.2–7.7) 9 2.3 (1.0–4.3) 4 1.2 (0.1–2.3) 13 1.8 (0.9–3.0) <0.001 ASC–US or worse 610 41.2 (38.7–43.8) 332 44.9 (41.3–48.5) 162 40.9 (36.0–45.9) 116 33.7 (28.7–38.7) 278 37.6 (34.1–41.2) 0.004 HPV-18 related (no 16) 77 5.2 (4.1–6.3) 51 6.9 (5.2–9.0) 19 4.8 (2.9–7.4) 7 2.0 (0.8–4.2) 26 3.5 (2.3–5.1) 0.003 Normal 13 0.9 (0.4–1.4) 9 1.2 (0.6–2.3) 4 1.0 (0.1–2.0) NA NA 4 0.5 (0.2–1.4) 0.164 ASC–US or worse 58 3.9 (3.0–5.0) 38 5.1 (3.7–7.0) 14 3.5 (1.7–5.4) 6 1.7 (0.4–3.1) 20 2.7 (1.5–3.9) 0.016 Abbreviation: CIN=cervical intraepithelial neoplasia; HPV=human papillomavirus;CI=confidence interval; ASC–US=atypical squamous cells of undetermined significance; NA=not available. Table 1.Prevalence of HPV types in cases with cervical intraepithelial neoplasia grade 1, 2, and 3.
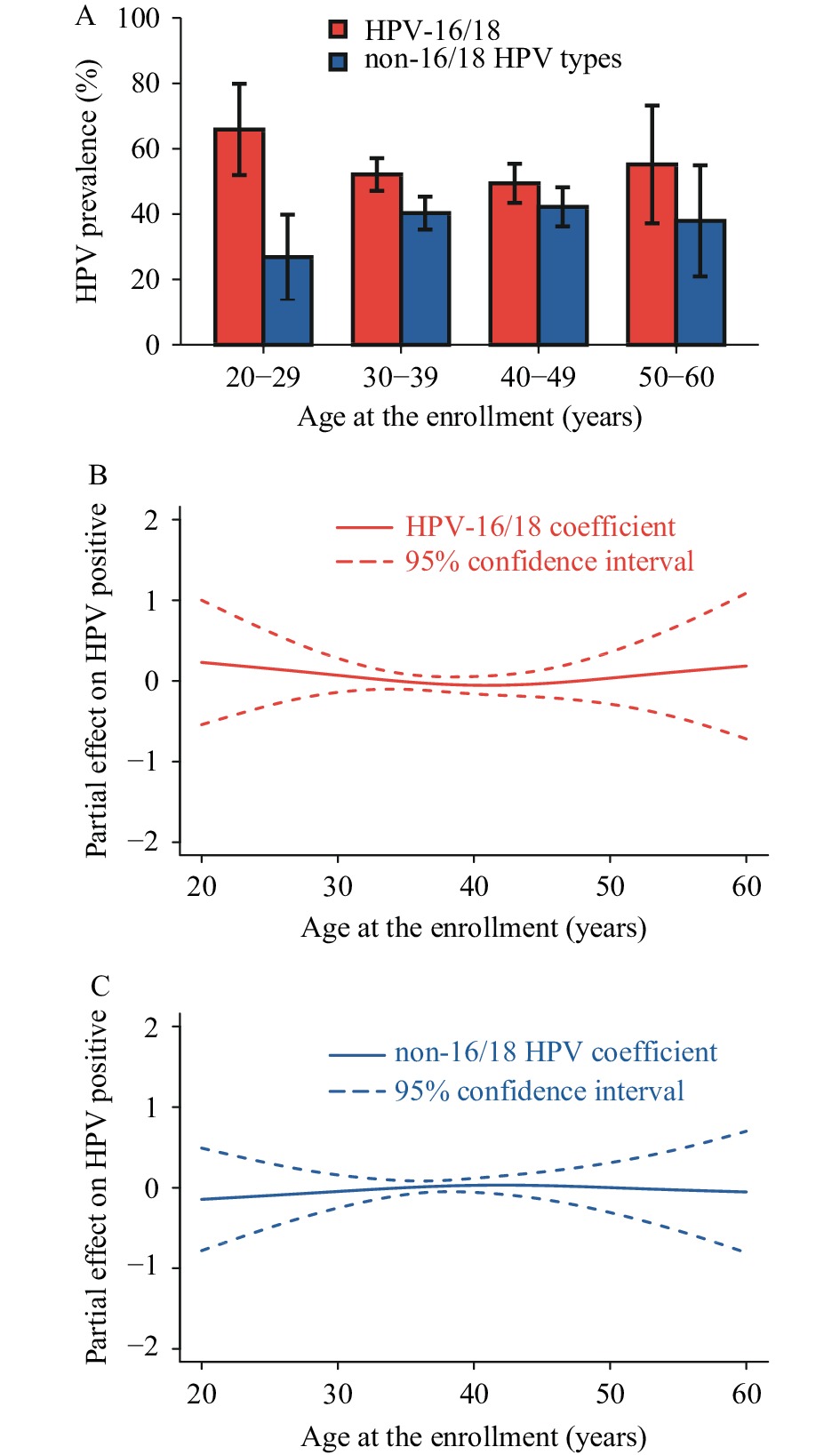
The age-specific HPV-16/18 prevalence in CIN2/3 ranged from 49.4% to 65.9%, and non-16/18 HPV type prevalence ranged from 26.8% to 46.2% (Figure 1A). The highest HPV-16/18 prevalence was observed in individuals aged 20–29 years, whereas the highest prevalence of non-16/18 HPV types was observed in individuals aged 40–49 years. Overall, the non-linear models revealed HPV prevalence was equivalent across age groups for CIN2/3 (Figure 1Band1C). Nonetheless, the association of HPV-16/18 with CIN2/3 was slightly more prevalent among younger (<30 years) and older (>50 years) women.
 Figure 1.
Figure 1.Age-specific HPV prevalence in cases with cervical intraepithelial neoplasia 2/3 and the association between HPV infection and age. (A) The prevalence of HPV-16/18 and non-16/18 high-risk HPV types in CIN2/3; (B) The non-linear association of age with HPV-16/18 positive in CIN2/3 cases; (C) The non-linear association of age with non-16/18 HPV types positive in CIN2/3 cases.
Abbreviation: HPV=human papillomavirus; CIN=cervical intraepithelial neoplasia.The pattern of HPV infection was associated with an increased risk of high-grade CIN to a different extent (Table 2). Ordinal multivariate analyses revealed that patients with HPV-16/18 and non-16/18 HPV types had increased odds of 5.5 (OR=5.51, 95%CI: 3.92–7.73) and 2.1 (OR=2.14, 95% CI: 1.54–2.99) of developing CIN2/3, respectively, compared to patients negative for HPV. Furthermore, HPV-16-related infection was associated with a 7-fold increased risk of developing CIN2/3 (OR=6.96, 95%CI: 4.92–9.84). These results remained stable in binomial multivariate analyses.
Model Dependent
variableOrdinal logistic regression
for CIN 1, 2, and 3Binomial logistic regression
for CIN2/3vs. CIN1Binomial logistic regression
for CIN3vs. CIN1/2OR(95%CI) P OR(95%CI) P OR(95%CI) P Model 1 HPV negative Reference Reference Reference Other HPV types
(no HPV-16/18)2.14 (1.54−2.99) <0.001 2.15 (1.54−3.02) <0.001 2.12 (1.28−3.50) 0.003 HPV-16/18 5.51 (3.92−7.73) <0.001 5.74 (4.04−8.15) <0.001 5.07 (3.09−8.32) <0.001 Model 2 HPV negative Reference Reference Reference Other HPV types
(no HPV-16/18)2.17 (1.55−3.02) <0.001 2.17 (1.54−3.03) <0.001 2.13 (1.29−3.52) 0.003 HPV-16 related 6.96 (4.92−9.84) <0.001 7.48 (5.19−10.76) <0.001 6.12 (3.71−10.08) <0.001 HPV-18 related
(no HPV-16)1.33 (0.76−2.31) 0.305 1.40 (0.80−2.46) 0.296 0.92 (0.37−2.29) 0.864 Abbreviation: CIN=cervical intraepithelial neoplasia; HPV=human papillomavirus;OR=odds ratio; CI=confidence interval. Table 2.Association of HPV infection pattern with high-grade cervical intraepithelial neoplasia in cases.
-
This 2017–2018 study obtained histological confirmations from almost 1,500 CIN cases and is therefore the largest study in China to report the prevalence of HPV types in CIN cases in the country’s pre-vaccine era. We estimated that more than 90% of CIN2/3 patients were positive for high-risk HPV, suggesting that HPV-focused strategies may be important for the prevention of cervical cancer. Furthermore, our results showed that HPV-16 and HPV-18 were significantly associated with an increased risk of high-grade lesions and that preventing these subtypes should be prioritized when designing cervical cancer vaccination and screening strategies.
Consistent with previous research, this study showed a high HPV prevalence (92%) in CIN and an association between high-risk HPV types and CIN2/3. These findings emphasize the importance of HPV-based screening and vaccination strategies to eliminate and mitigate cervical cancer in China. In this study, the HPV prevalence in CIN2/3 was slightly lower than in the previous multicentric study of China in 2009 (94.2%vs. 98.9%) (4). Both studies tested all high-risk HPV types and indicated the importance of HPV-based strategies for prevention of CIN. However, HPV-16 prevalence decreased by approximately 30% in CIN2/3 patients in our more recent study (48.5%vs. 68.7%). Given that HPV vaccination has not been implemented in the population, the reduction may be related to screening and subsequent treatment, which would protect against subsequent HPV infection by antigen-presenting effects (6). Our results showed a low prevalence of HPV-18 in CIN2/3 patients and anORwithout significance. This could be explained by a smaller number of AIS cases in the study. Adenocarcinoma accounted for a small proportion of cervical cancer but was closely related to HPV-18 infection (7-8).
The proportion of non-16/18 high-risk HPV types in CIN2/3 was higher than in the study in 2009 (4). Although these non-16/18 HPV types have a lower risk of CIN2/3 than HPV-16/18, they are predominant in Chinese women, particularly HPV-52 and -58 (9). After the application of bivalent vaccines and screening based on HPV-16/18, these HPV types would gradually change to the predominant types. Among the CIN2/3 cases with non-16/18 HPV type positives, 1.8% were classified as normal cytology CIN2/3 and would be missed in the screening. Thus, primary HPV screening with HPV-16/18 genotyping was feasible but new stratification technology should be developed to reduce underdiagnosis.
The bimodal pattern of HPV prevalence in the population was identified by many studies in China (9-10). Nonetheless, our age-specific analyses showed that the roles of different HPV types were equivalent across the age spectrum. Furthermore, these results indicate that HPV vaccinations before the age of 20 should provide benefits that last until patients are 60 years old.
The key limitation was that results for HPV infection were from cervical scraping rather than paraffin-embedded biopsy specimens, which could lead to misclassification bias or false-negative results. A small spectrum of 14 HPV types also increased the likelihood of false negatives. Nonetheless, a high-sensitive PCR-based assay would reduce the risk of misclassification, and the proportion of HPV-negative CIN2+ in our study was similar to previous studies (11-12).
In conclusion, HPV-based screening and HPV vaccination strategies greatly influence the prevention of cervical cancer in China. HPV-16 and HPV-18 should be priority vaccinations in China, and the prevention of non-16/18 high-risk HPV types will be essential to eliminate cervical cancer in the future.
-
All research staff from the hospitals and health centers associated with this project.
-
No conflicts of interest.
HTML
| Citation: |

|